
Fetal alcohol syndrome disorder is a spectrum of physical, cognitive, and behavioral impairments that result from prenatal alcohol exposure. Early alcohol exposure before birth can inhibit the proper development of the brain, which eventually results in a spectrum of physical and cognitive impairments.
The dose, pattern, timing, and duration of maternal alcohol exposure during pregnancy determine the level of exposure and effect. There is no specific safe quantity of alcohol to take during pregnancy, as both heavy and light alcohol intake could potentially result in fetal alcohol spectrum disorder (FASD). The effects of these disorders can span the lifetime of the child affected if detected late. Approximately 1% to 5% of first graders in the USA have fetal alcohol spectrum disorder.
In this article, the cause, treatment, prevention, and early detection modalities of the fetal alcohol spectrum will be explained. Awareness and early intervention are important, as they help to mitigate the consequences associated with the lifelong disease process.

Definition and Scope of FASD
FASD Meaning
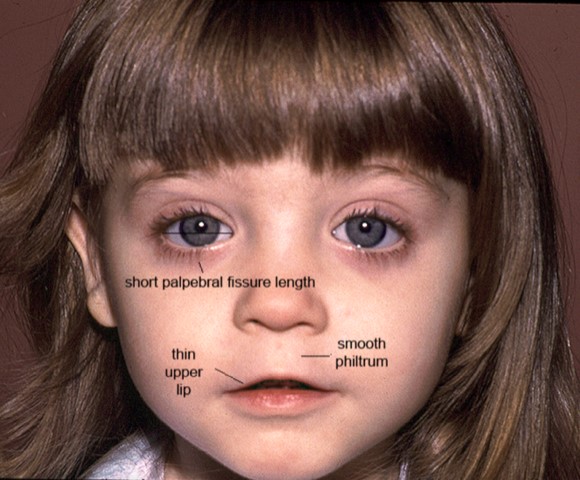
Fetal alcohol spectrum disorder (FASD) is a range of conditions exhibited by physical, behavioral, and cognitive problems associated with prenatal alcohol exposure. This spectrum has different presentations, especially as it impacts the brain. A common feature is the presentation of the fetal alcohol syndrome face, which is seen as a smooth philtrum, a thin upper lip, an upturned nose, a flat nasal bridge and midface, a small head circumference, and small palpebral fissures.
Types of FASD
Different categories can be used to classify fetal alcohol spectrum disorder. Here are some types and their manifestations:
Fetal Alcohol Syndrome (FAS)
This is on the severe side of the spectrum. It involves both neurodevelopmental and physical impairments. The FASD facial features associated with this type include reduced palpebral fissures, a smooth philtrum, and a thin upper lip. These facial features, among other characteristics, indicate a lower-than-average height, weight, head circumference, and neurocognitive signs of a neurodevelopmental deficit.
Partial Fetal Alcohol Syndrome (pFAS)
This is quite uncommon when compared to fetal alcohol syndrome. Some facial and growth abnormalities are present, but not to the extent of fetal alcohol syndrome (FAS) in this case.
Alcohol-Related Neurodevelopmental Disorder (ARND)
This involves only the neurodevelopmental and neurobehavioral aspects of the spectrum. It is fetal alcohol syndrome, minus the physical abnormalities.
Alcohol-Related Birth Defects (ARBD)
The features of this alcohol fetal syndrome are more congenital abnormalities involving the bones, heart, and kidneys, as well as hearing and vision anomalies with no neurodevelopmental abnormalities.
Summary of FASD Categories and Characteristics
| FASD Category | Characteristics |
| Fetal Alcohol Syndrome (FAS) | Physical and neurodevelopmental abnormalities such as fetal alcohol syndrome of the face, lower than average height, weight, and head circumference. |
| Partial Fetal Alcohol Syndrome (pFAS) | Presence of some features seen in FAS that affect facial growth but are not diagnostic for FAS. |
| Alcohol-Related Neurodevelopmental Disorder (ARND) | Neurodevelopment and neurobehavioral abnormalities with no physical anomaly. |
| Alcohol-Related Birth Defects (ARBD) | Presence of congenital anomalies involving the bones, heart, and kidneys with no neurodevelopmental affectation. |
Causes and Risk Factors
Different evidence and presentations can debate the actual cause and determining factors for fetal alcohol spectrum disorder. Alcohol use can cause fetal alcohol syndrome in the unborn fetus. True or false. Definitely true. The consumption of alcohol by the mother impedes the normal development of the brain and related structures in the fetus, resulting in fetal alcohol spectrum disorder upon birth.
The severity of FASD’s presentation depends on some specific risk factors. These factors can exacerbate the presentation of this disorder if not properly managed. Here are some risk factors:
- Amount and frequency of alcohol intake: Heavy alcohol use during pregnancy poses a great threat to the fetus. This quantity of alcohol can greatly affect the developmental process of the baby, leading to more intense FASD symptoms.
- Timing during pregnancy: The different trimesters are important for the growth of different body parts. Exposure to alcohol during these specific periods has different effects. In the first trimester, when the brain is developing, the most severe exposure presentation is observed.
- Genetic predispositions: If a woman has a genetic predisposition to metabolize alcohol slowly, she can have more severe impacts on the fetus if she consumes alcohol. This is because it will take longer to eliminate alcohol from the body, which prolongs its effect on the fetus.
- Maternal health and nutrition: The mother’s health during pregnancy is quite important. It can affect the way the maternal body system responds to its protective possibilities for fetal health. Poor nutrition can greatly affect the fetus in general, making it more difficult to respond to alcohol exposure in utero adequately.
- Socioeconomic factors: Early detection and intervention are important for the baby at birth. In low-socioeconomic environments, the response to this can be slow and inefficient, resulting in more fatal outcomes.
Signs and Symptoms of FASD
The clinical presentation of FASD is distinct from the evidence showcased in the form of physical, cognitive, behavioral, and neurological anomalies. Here are some FASD signs and symptoms:
Physical Effects
A distinct feature seen in FASD is its physical anomalies. Although not seen in all types of fetal alcohol spectrum disorder, it plays a major role in identifying this condition. FASD features are commonly seen as fetal alcohol syndrome baby face, with the following characteristics:
- Smooth philtrum
- Thin upper lip
- Upturned nose
- Flat nasal bridge and midface
- Epicanthal folds
- Small palpebral fissures
- Small head circumference
Infants exhibit these facial features to varying degrees with the disorder. In older children, there could be additional low growth for age, a malnourished body even in children with a good diet, drooping of one or both eyelids, and hearing and vision loss.
Photos of the FAS Baby Face

Cognitive Impairments
Individuals with FASD exhibit neurocognitive anomalies due to the improper development of their brains. A lower intelligence quotient, reduced memory retention, and impaired learning ability can be seen as signs of this.
Behavioral and Emotional Challenges
Emotional maturity is a great deal for individuals with FASD. There is evidence of trouble controlling emotional impulses, defective communication, and social skills, and negative hyperactive behavior.
Secondary Disabilities and Associated Conditions
Additional impairments seen in individuals with FASD range from an inability to have effective motor coordination to lifelong dependency and mental health issues.
Symptoms of FASD in Adults
Fetal alcohol syndrome adults symptoms are a progression of childhood manifestations of FASD. These symptoms can, however, affect other aspects of life, resulting in long-term outcomes such as high rates of dependency, a lack of motor coordination, dyslexia, a low intelligence quotient, and mental health issues such as attention deficit hyperactivity disorder (ADHD), depression, and suicidal attempts.
Fetal Alcohol Syndrome Face Photos in Adults


Diagnosis of FASD
A pediatrician carefully uses a comprehensive history and clinical methods to diagnose fetal alcohol spectrum disorder in its early stages. The challenges associated with the diagnosis of this disorder can be a result of inadequate history, especially in foster/adopted children. The confirmation of prenatal alcohol use plays a major role in the early diagnosis of this disorder.
Diagnostic Criteria for FASD
The diagnosis of fetal alcohol spectrum disorder requires the use of three levels of assessment to determine the role of alcohol in the development of a fetus.
- Medical history and maternal alcohol consumption: History-taking gives a background understanding of what the prenatal life of a child looks like. To make a diagnosis of FASD, there must be a positive history of maternal alcohol consumption during pregnancy.
- Physical examination: The pediatrician clinically assesses the physical features of FASD during a physical examination. This will help to provide a second level of confirmation after a history of prenatal alcohol use. The facial features are the most distinct features seen in FASD, depending on the type seen in an individual.
- Neuropsychological assessments: Neurodevelopmental assessment is the third level of confirmation needed to make a diagnosis of FASD. This assessment will look at brain structure, attention deficit hyperactivity, motor skills, and cognitive behavior.
The advantage of having this diagnosis made early is that it will help to efficiently provide adequate intervention necessary to help the life of the child.
Treatment and Support
There is no specific cure, but treatment modes involve factors such as early diagnosis and peculiar support for education to reduce the effects of FASD, help them maximize their full potential, and prevent secondary disabilities. Treatments must specifically address the individual’s disability to be effective. These can include:
- Medical management, which involves medications for anxiety, hyperactivity, and poor focus; health care professionals for vision, hearing, or heart conditions; and mental health professionals for mental disabilities.
- Early intervention therapists such as speech, physical, and occupational therapists for walking, talking, and social skills.
- Early intervention programs: This is a special program applicable to children under 3 years of age with FASD. Here, skills such as walking and social interaction are addressed. Children are often evaluated, and their needs are assessed through screening processes.
- Educational and behavioral therapies: Behavioral therapies really help children with FASD deal with challenges in their behavior as they grow. Parents must keep instructions simple, be very patient, set limits and stick to them, keep them on a routine, repeat teaching to reinforce learning, reward positive behaviors, and protect their kids.
- Family support and resources: This involves receiving help and counsel from other families who have experience with this condition. Social workers and counselors are also helpful here.
Prevention and Intervention
To prevent FASD or provide early intervention, there are key things that need to be put in place.
Preventing Alcohol Use During Pregnancy
The best method of preventing FASD (Fetal Alcohol Spectrum Disorder) is to avoid consuming alcohol while pregnant. If you are not trying to get pregnant, properly use condoms, contraceptive pills, and other well-proven means of contraception if you are having sex and drinking alcohol. However, about 50% of pregnancies are unplanned, and people have consumed alcohol before even realizing they are now pregnant.
If alcohol cessation seems too difficult to handle, seeking support from people can be of great assistance. Support from health care providers such as doctors, nurses, midwives, therapists, primary health centers, other family members, and friends. While alcohol intake by one’s partner will have no effect on the baby, one can also stop taking alcohol to provide support for the birthing partner.
Early Identification and Diagnosis
Although numerous other conditions make it difficult to diagnose fetal alcohol spectrum disorders before or after birth, the diagnosis itself is challenging. The most seriously affected children can be diagnosed with FASD at birth. Their physical characteristics become most noticeable between the ages of eight months and eight years. Children with FASD often develop much slower than expected for their age, and such presentations should call for more in-depth examinations to rule it out. Early detection allows for early intervention, which reduces the chance of negative adolescent or adult outcomes by two to four times. These outcomes include disrupted schooling, legal issues, incarceration, recurrent improper sexual behavior, social disorders, and alcohol and drug abuse.
Educational and Behavioral Interventions
People with FASD can receive special education assistance since the education system has incorporated support for FASD. The change in education regulations now lists FAS under the special education category “Other Health Impaired. In addition to doctors, this policy broadens the pool of people who may diagnose medical conditions by including advanced-practice registered nurses. Children with FASD may be referred automatically for special education assistance and receive treatment under Section 504 of the Rehabilitation Act of 1973 or an Individualized Education Plan (IEP), depending on the evaluated need’s degree.
Public Health Campaigns and Education
Many FASD prevention campaigns exist, targeting pregnant women or those planning to get pregnant. These use varying materials, such as posters and brochures, websites, radio, and TV announcements, to educate the populace about FASD and its associated causal factors.
- ‘Pregnant? No Alcohol’ campaign teaches that no amount of alcohol is safe during pregnancy.
- SAMHSA developed ‘Alcohol and Pregnancy’ to teach that FASD is 100% preventable.
- ‘Infinite power’ emphasizes that the power to prevent FASD belongs to women.
- ‘Together we can prevent FASD’ talks about the supportive roles of family and friends in alcohol cessation during pregnancy.
Policy Recommendations
There are currently neutral policies like warning signs about drinking during pregnancy posted in retail stores and limits on prosecution for positive toxicology screens; supportive policies like priority SUD treatment for pregnant women; and civil commitment and mandatory reporting by health care workers and social workers of pregnant women who are actively using alcohol. Policy suggestions suggest that packaging alcoholic beverages with pregnancy warning labels should develop and include a pictogram and relevant warning statement as a mandatory requirement. Women of childbearing age should receive more education on pregnancy prevention and family planning using effective contraceptive tools.
Societal Impact and Awareness
Economic Burden of FASD
FASD places a huge financial burden on families, individuals, and society at large. One child with FASD and one adult require approximately $22,000 and $24,000, respectively, yearly for their care. There are huge burdens on correctional facilities, as evidenced by the over-representation of individuals with FASD. Adolescents who have FASD are 19 times more likely to be incarcerated than those who do not have it. Caregivers of individuals with FASD lose a lot of productivity time due to the care required by their conditions. Recommendations have been made to spend more efforts on prevention policies due to the enormous costs associated with this condition, which is highly preventable.
Stigma and Misconceptions
Many misconceptions exist about FASD:
- A diagnosis does no good, as there are no treatments available
- They all have low IQ
- They are completely unable to live a normal life
- It goes away as people age
- Poverty is a major cause
- Some levels of alcohol in pregnancy are safe and the placenta will protect the fetus
These misconceptions do more harm than good; some trivialize the struggles people with FASD undergo, and others prevent people from seeking appropriate assistance. People dealing with FASD alongside their families also deal with stigmatization at different levels.
Healthcare providers have been found to judge mothers for their alcohol consumption during pregnancy; some others refuse to treat the guardians of special needs individuals with empathy, knowing that they are probably under a certain level of stress. People are discouraged from seeking treatments for these findings.
People with FASD (Fetal Alcohol Spectrum Disorders), due to their lifelong disabilities, are often misunderstood, isolated, and discriminated against in societal norms.
Conclusion
The burden of FASD is a huge one, on the individual who played no part in its development, their caretakers, and society at large. Most of this disability is hidden within the brain and in the minds of those who suffer from it. Society strongly discriminates against the disabilities associated with FASD while refusing to acknowledge its contributory roles. Many treatment options are available and must be administered. Many challenges face the complete prevention of FASD. No preventive measures will be too enormous to undergo, as the potential for success is enormous.